

A&E chock-a-block. “Overspend” of £26m. Threat to “shuttle bus”
This week we have been presented with a couple of “crisis” issues facing the East Lancashire Hospitals NHS Trust, and Blackburn A&E.
The situation at A&E in Blackburn received regional and local press attention, with reports of patients having to wait up to 15 hours.
In a separate development, the Chief Executive of the Trust wrote to all staff to say that the Trust is currently running at a £26m overspend and that it was “under a programme of system-level investigation and intervention, with an unequivocal mandate to reduce costs with immediate effect“. The intention was “focus on discharges across every area as a priority, reducing our bed occupancy before Christmas” and to adopt a range of further measures, such as:
- A hold all on vacancies for a minimum of 12 weeks with very few exceptions based only on critical requirements
- A stop on all non-essential spending for every team without exception
- A pause on non-essential educational activity to help reduce costs and enable colleagues to remain in their roles, removing the need for expensive bank or agency cover
- Reducing or stopping completely any activity that the Trust is not funded for
- Ensuring everything we do is appropriately and effectively coded and charged
- Reconsidering any activity which is not within our core business and within this likely changes to provision such as the shuttle bus
Some interplay is seen between the two issues, insofar as the Trust CEO describes the A&E situation as “a key area where we are spending enormous amounts of energy and money”. But there are also ways in which the two things are separate.
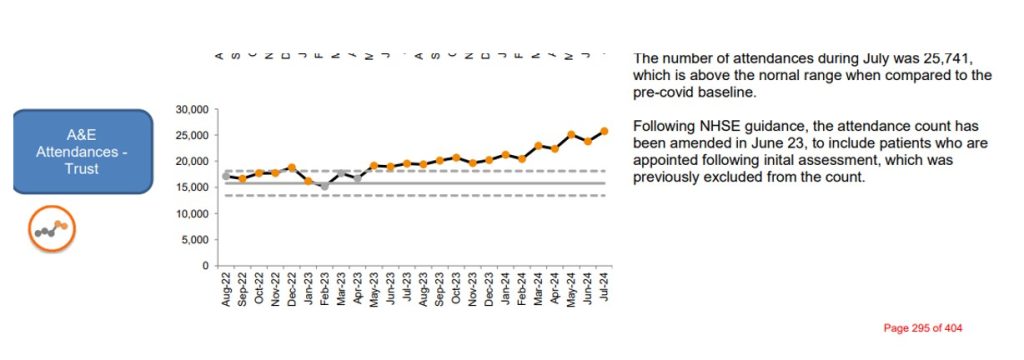
One side of the A&E situation is that demand on the department is showing a continuous upward trend.
Across the NHS there is a basic strategic idea is that this type of situation could be avoided if only people would change their behaviour. The East Lancashire Hospitals Trust Facebook page advises: “If your condition isn’t life or limb threatening and you can avoid going to A&E by either visiting your GP surgery, going to a local pharmacy or contacting NHS 111 for advice, that could potentially prevent you having a long wait”. The Integrated Care Board refers to “alternatives to Emergency Department Streaming, redirection and admission avoidance”. But, as we wrote to them in May, this strategy “seems to be evidently flying in the face of reality. On the one hand, public expectations are deeply engrained. On the other, people will only turn to alternatives when they have confidence in them” (May meeting – Trades Council voices A&E concerns – Blackburn and District Trades Union Council).
Significant knock-on effects come from:
a) the growing perception (justifiable or not) that there are obstacles to getting attention from a GP and
b) lack of public confidence in NHS111.
For so long as these exist there will doubtless remain a capacity issue – which the public locally will inevitably link to the historic reduction of services at Burnley and Chorley, and which might, in the medium term, only be addressable by reversing this.
Meanwhile, it is probably worth asking if there are knock-on effects specifically from the condition of community mental health services. The Care Quality Commission has reported that “people’s experiences of NHS mental health services provided in the community are poor”: Community mental health survey 2023 – Care Quality Commission. One way in which this might impact A&E services is through “Frequent Attendance”.
The Royal College of Emergency Medicine “Best Practice Guideline – Frequent Attendance in the Emergency Department” says that “The number of patients frequently attending EDs as a result of unmet health and care needs, or with underlying vulnerabilities is rising. An ED visit is not always beneficial for these patients and may increase heath care anxiety. Frequent attendance to the ED is often a reflection of a system wide deficiency of care for the most vulnerable members of society and this patient group has often been marginalised in the ED and other healthcare settings”. It also says that “…65% had mental health symptoms, 15% had significant alcohol problems, and 45% had medically unexplained symptoms. Patients with multiple vulnerabilities (e.g. chronic mental health problems combined with social problems and alcohol/substance misuse) are more likely to have the highest intensity of ED use and may struggle to access other services” and that “Given the increased prevalence of psychiatric disorders and alcohol misuse in this group of patients, challenging behaviour can be more common”.
There is some national recognition of this issue (Repeat A&E patients can account for almost one in seven visits | Lancashire Telegraph). A question could be raised, however, of whether there is any local work to monitor and, if possible, address it. It does not seem to get much of a mention at either Trust or ICB level.
It is not so easy from Board papers to get a clear view of the extent to which discharges are a problem leading to “back-up” in A&E.
The Trust’s “Risk Register” as presented at the last Board meeting (Increased demand with a lack of capacity within ED can lead to extreme pressure and delays to patient care) did say that: “limitations of ‘pull through’ and what can be achieved are due to challenges regarding patient discharge”. The NHS Statistics » Discharge delays (Acute) , however, suggest that the “discharge” is not as “bad” in East Lancs as elsewhere. The big worry with any “accelerated throughput” measure is that it might lead to patients being turfed out earlier than would be best for them.
Blackburn’s MP, Adnan Hussain, says he has received assurances that “the hospital is not understaffed, and all nurse vacancies have been filled”. Staffing levels are probably not a principal contributor to the congestion of A&E – but Board papers do suggest that there are problems where workload exceeds the levels on which staff establishments are based. The basic capacity issues thus create negative feedback in terms of care quality and “immediate” staffing. The “Risk Register” mentioned above said:
“A lack of capacity is leading to extreme pressure resulting in delayed delivery of optimal standard of care. At times of extreme pressure, increasing patient numbers across the emergency pathway makes the provision of care difficult, impacts on clinical flow, increases the risk of nosocomial infection spread as a result of overcrowding and poor patient experience leading to complaints.
“Staffing requirements are not calculated as standard to be able to care for increased patient numbers and complexity, with inadequate capacity within specialist areas such as cardiology, stroke etc. to ensure adequate clinical flow and optimum care”.
It also notes that: “further in reach to department support does not always occur due to staffing levels and space constraints” and that “staff are not always available to redeploy to support at times of increased pressure”. In broader terms, the “Integrated Performance Report” delivered to the Trust Board in September 2024 did say that average fill rates for registered nurses/midwives and care staff remained above threshold, but it also said the “the Trust vacancy rate is above threshold at 7.5%” and that “temporary costs as % of total pay bill remains above threshold at 13%”.
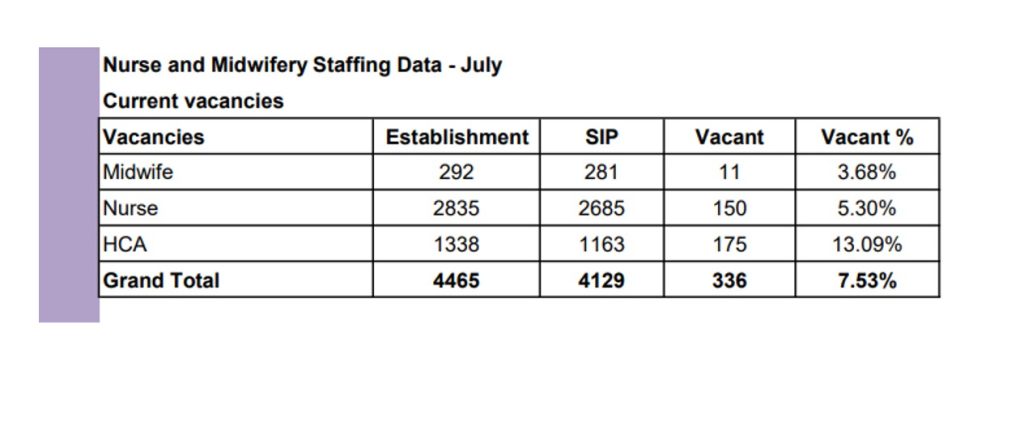
These figures may have varied since then and the Trust has subsequently said that it has taken on all newly qualified nurses, but that would not impact the HCA situation, where the vacancy percentage was highest. There remains cause for concern that this is not a scenario in which it is helpful to be talking in terms of “a hold on all vacancies for a minimum of 12 weeks”. It will be interesting to see what the situation is reported to be at the January Board meeting.
The “overspend” at the Trust appears to be a good example of how “efficiency savings” are really a sleight of hand expression for inadequate funding – you give with one hand and then take away with the other.
It is difficult to know at the best of times how to calculate the “ideal” allocation for a service, but the situation gets even worse when what is allocated is chipped away at by other measures. The Trust Board itself notes that it has been asked to meet a “7.7% efficiency target of £57.8m” …… “a level that has never been achieved previously”. It also says the “overspend” is due to ” industrial action and a shortfall in funding for consultant pay award on addition to additional ward areas being used, corridor care staffing, pathology and security management costs and additional waiting lists in surgery”. According to “We Own It”, Tony Blair’s Private Finance deals still haunt the NHS, new league table reveals | We Own It, the Trust is also saddled with £1.1bn PFI payments from May 2006 — Jul 2041.
Other than the “go slow” on vacancy filling, it is very difficult to pin down what the Trust’s “expenditure reductions” will actually amount to – except that the “shuttle bus” has clearly been put in the firing line again as a “low hanging fruit” (our term, not theirs). It seems to be a classic case of bosses picking on something they don’t really understand the value of because they have never really understood how helpful it is. The feedback we get is that this service is still valued by staff, visitors, and patients and that staff have, in the past, agreed to switch between the main hospital sites because it was there to help them get to and from their proposed new assignment.
The best immediate measures the government could take to alleviate the situation are:
- To abolish the “efficiency savings” and provide Trusts with the allocation they are owed, and
- To take central responsibility for all PFI payments.
Meanwhile we will need to do what we can to defend service levels locally.